
Shoulder Impingement Relief: Stop Pain & Restore Movement
Persistent shoulder pain with overhead activities, painful arc when lifting your arm, and nagging discomfort that disrupts sleep these are the hallmark signs of shoulder impingement syndrome. This common condition occurs when the rotator cuff tendons and bursa are pinched in the narrow subacromial space between your arm bone and shoulder blade, causing inflammation, pain, and progressive weakness. Dr. Usama Saleh, Dubai’s fellowship-trained shoulder specialist with 23+ years of experience, provides comprehensive shoulder impingement treatment starting with conservative care physical therapy, targeted shoulder impingement exercises, and anti-inflammatory injections achieving excellent relief for 70-80% of patients.
Understanding
Shoulder Impingement
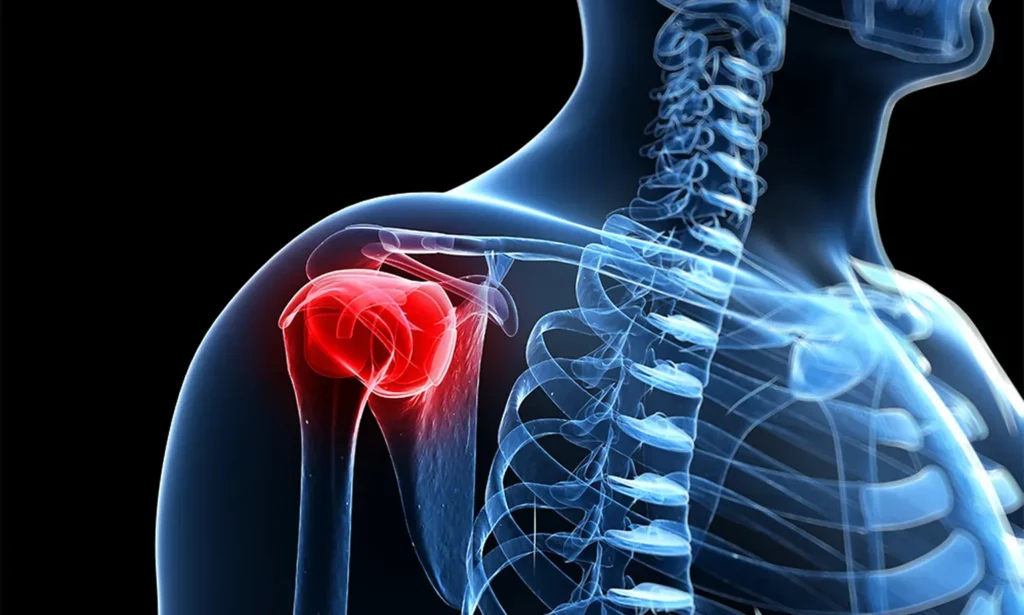
Shoulder impingement syndrome, also called subacromial impingement, occurs when the narrow space beneath the acromion compresses critical joint structures.
This mechanical pinching happens repeatedly during arm elevation, particularly between 60-120 degrees (the ‘painful arc’). The compression directly affects the rotator cuff tendons (primarily the supraspinatus tendon) and the subacromial bursa.
If left untreated, this constant friction leads to severe tendon inflammation (tendinitis), bursa inflammation (subacromial bursitis), and progressive tendon degeneration.
Why Does the Subacromial Space Narrow?
The space diminishes due to bone spurs on the underside of the acromion (common over 40), thickened inflamed bursa, rotator cuff tendon swelling from overuse, poor posture, and muscle weakness allowing the humeral head to migrate upward.
What causes shoulder impingement? Usually a strategic combination of anatomic factors (bone spur shoulder shape, acromion anatomy) and mechanical factors (poor technique, muscle imbalance, overuse).
Shoulder Impingement Symptoms
Early identification of mechanical compression path mechanisms optimizes tracking recovery. Symptoms diverge strictly between acute flares and degenerative chronic progressions.
Primary Symptoms Scan
Painful Arc Sensation
Sharp pinching pain triggered explicitly when elevating the arm between 60-120 degrees overhead.
Deep Joint Aching
Continuous deep aching concentrated in the front and lateral fields of the shoulder architecture.
Nocturnal Flare-ups
Severe pain aggravation when lying on the affected joint, leading to persistent sleep disruption.
Functional Weakness
Pronounced mechanical difficulty when lifting heavy objects overhead or reaching behind the spinal column.
Clinical Presentation Spectrum
Sudden onset following unaccustomed overhead loads. Symptoms typically mitigate with rest and exhibit high compliance with non-surgical metrics.
Gradual onset spanning months with progressive resistance to rest. Highly correlated with subacromial bone spurs or advanced tendon wear.
Clinical Red Flags
Immediate evaluation by a shoulder specialist doctor is essential if tracking any of the following parameters:
- Sudden absolute loss of arm elevation strength after sudden strain (Possible complete tear)
- Debilitating acute pain restriction during minimal non-loaded movements (Possible calcific tendinitis)
- Zero clinical symptom modification after 6-8 weeks of dedicated conservative care
- Progressive, continuous muscle atrophy and weakness despite ongoing therapy
How Is Shoulder
Impingement Diagnosed?
Precision diagnostics guide optimal treatment. Dr. Usama combines targeted functional tests with advanced multi-modal imaging to measure subacromial space restrictions accurately.
Board certified in orthopedics surgery
Clinical Examination
Dr. Usama performs highly sensitive shoulder impingement tests (75-90% sensitivity). This includes the Neer Test and Hawkins Test to reproduce mechanical pinching, the Painful Arc Test (pain between 60-120 degrees), the Jobe Test to isolate supraspinatus health, and the Drop Arm Test to evaluate structural tendon tears.
Imaging & Confirmation
X-rays & MRI: Initial X-rays evaluate bone spurs and calcific deposits, while MRI serves as the gold standard for checking tendon degradation and bicep/bursa thickness.
Ultrasound & Lidocaine Testing: Ultrasound allows dynamic tracking of tendon gliding, while a subacromial lidocaine diagnostic injection test confirms the clinical diagnosis if immediate pain resolution is achieved.








Treatment Options For Shoulder Impingement
How to treat shoulder impingement depends on severity, duration, structural factors, and your individual response to initial clinical care.
Dr. Usama’s Clinical Approach: Emphasizes conservative shoulder impingement treatment first for 3-6 months (successful in 70-80% of cases). Surgical intervention is strictly reserved for instances when conservative care fails or structural bone spurs cause definitive mechanical impingement.
Conservative Treatment (First-Line)
Shoulder Impingement Physical Therapy
A dedicated 12-16 week program focusing deeply on rotator cuff strengthening, scapular stabilization, posterior capsule stretching, and kinetic posture correction. This operates as the absolute baseline of non-surgical resolution.
Corticosteroid Subacromial Injection
Targeted anti-inflammatory relief that effectively reduces bursa inflammation, providing 6-12 weeks of pain alleviation to allow patients to participate effectively in active physical therapy. Can be repeated 2-3 times if indicated.
Short-Term Adjunct Care
Utilization of NSAIDs for a short-term window of 7-14 days to manage acute flare-ups, combined with temporary guided activity modification to prevent constant mechanical pinching.
Surgical Intervention (Advanced)
Arthroscopic Subacromial Decompression
An advanced minimally invasive procedure performed through 2-3 tiny incisions. The technique cleanly removes offending bone spurs from the acromion, excises the chronically thickened bursa, and smooths out any minor rotator cuff fraying.
Surgery Is Only Recommended When:
- Failed 3-6 months of structured conservative treatment.
- Structural bone spurs are confirmed via diagnostic imaging.
- Progressive, compounding rotator cuff tendon degeneration.
- Significant functional limitation disrupting daily life parameters.
What Causes Shoulder Impingement?
Understanding the precise mechanical and anatomical triggers optimizes targeted treatment strategies and long-term prevention protocols.
Mechanical Triggers
Bone Spurs & Anatomy
Acromion bone spurs (common in adults 40+) and a hooked acromion shape mechanically narrow the subacromial space, pinching the rotator cuff. These structural overgrowths do not resolve conservatively and typically require surgical removal.
Rotator Cuff & Bursa Inflammation
Repetitive overhead activity causes tendon swelling and shoulder bursitis. An inflamed subacromial bursa takes up vital joint space, worsening the mechanical pinching in a vicious cycle. Reversible with early targeted therapy.
Poor Biomechanics
Scapular dyskinesis (abnormal shoulder blade movement), rounded posture, and rotator cuff weakness allow the humeral head to drift upward. These functional causes are highly correctable with specialized physical therapy.
Clinical Risk Factors
A patient's overall structural risk metrics increase significantly when matching any of the following clinical parameters:
Exercises & Conservative Care
Shoulder impingement exercises are the most important component of conservative treatment. They must be performed with perfect precision, as improper mechanics worsen structural compression.
Clinical Focus Matrix: Every protocol centers strictly on strengthening the rotator cuff muscles, stabilizing the scapula, deeply stretching the tight posterior capsule, and correcting kinetic posture architecture.
Shoulder Impingement Exercises (12-Week Protocol)
Pain Control & Gentle ROM
Rotator Cuff Strengthening
Functional Strengthening
Pain Control & Gentle ROM
Rotator Cuff Strengthening
Functional Strengthening
Exercise Cautions & Safety Controls
STOP IMMEDIATELY if you experience sharp pain, increasing pain after a session, or compounding worsening of symptoms.
When Is Surgery Needed?
Most shoulder impingement cases respond effectively to non-surgical measures. Surgery is carefully considered only when specific clinical thresholds are met.
Surgical Criteria
Surgery is explicitly considered when structured conservative treatment has been comprehensively attempted for 3-6 months with strict compliance, mechanical bone spur impingement is confirmed on X-ray, progressive tendon degeneration tracks on MRI despite active therapy, or recurrent symptoms continuously limit daily work and sports metrics. Dr. Usama ensures surgery is truly needed before recommending it.
Success Metrics
Conservative Success Rate: 70-80% of patients achieve significant structural relief within 3-6 months of dedicated high-compliance therapy.
Surgical Success Rate: 85-90% achieve good-to-excellent predictable outcomes when properly indicated. Key Point: Surgery is never a first-line path unless rare, severe mechanical spur blocks exist.
Surgical Execution
Arthroscopic subacromial decompression systematically removes bone spurs, excises the chronically inflamed bursa, and smooths out the frayed fields of the rotator cuff. For complete step-by-step techniques, risks, complications, and comprehensive protocols, please refer to our dedicated Subacromial Decompression procedure page.
Recovery & Healing Time
Shoulder impingement recovery time depends heavily on the treatment approach, pathology severity, and patient compliance. How long it takes to heal varies by individual factors.
Why Choose Dr. Usama
For Shoulder Impingement Treatment In Dubai
Best Shoulder Doctor Dubai — Fellowship-Trained
23+ Years as Dubai's Shoulder Specialist Doctor
Expert in How to Treat Rotator Cuff Tear — All Options
Honest — Surgery Only When Truly Needed
Frequently asked questions
Need something cleared up? Here are our most frequently asked questions.
Shoulder impingement syndrome is compression and inflammation of the rotator cuff tendons and bursa in the subacromial space, the tendons are irritated but intact. A rotator cuff tear is actual tearing of the tendon fibers, partial or complete. However, these often coexist: chronic untreated impingement progressively damages tendons leading to tears (Stage 3 impingement). Impingement symptoms: painful arc shoulder, night pain, weakness but can lift arm. Rotator cuff tear symptoms: similar but often more severe weakness, sometimes inability to lift arm depending on tear size. MRI distinguishes between the two. Treatment differs: impingement primarily conservative, large tears often need surgery.
Yes, 70-80% of shoulder impingement cases heal with conservative treatment, physical therapy, shoulder impingement exercises, anti-inflammatory measures, and activity modification. How long does shoulder impingement take to heal without surgery? Typically 12-16 weeks of dedicated therapy. Factors favoring non-surgical healing: acute onset (caught early), no significant bone spurs on X-ray, good rotator cuff tendon quality on MRI, patient compliance with therapy, addressing biomechanical factors. Surgery only needed when: bone spurs cause mechanical impingement, conservative treatment failed after proper 3-6 month attempt, progressive tendon degeneration, work/sport demands require it.
The best exercises for shoulder impingement focus on three areas: (1) Rotator cuff strengthening: external rotation with resistance band, internal rotation exercises, strengthens dynamic stabilizers preventing upward humeral head migration. (2) Scapular stabilization: scapular retraction exercises, wall slides, rows, corrects poor shoulder blade mechanics contributing to impingement. (3) Posterior capsule stretching: cross-body stretch, sleeper stretch, tight posterior capsule alters mechanics and worsens impingement. Shoulder impingement stretches are essential component. CRITICAL: proper technique is essential, improper exercise worsens impingement. Work with physiotherapist experienced in shoulder conditions for proper progression. Avoid: overhead pressing, heavy lifting, exercising through pain.
Frozen shoulder vs impingement: Key differences are: Range of motion, impingement has good passive ROM (someone else can move your arm fully), frozen shoulder has severely restricted passive ROM (even when relaxed, arm won't move). Painful arc shoulder, impingement has painful arc between 60-120 degrees, frozen shoulder has global pain and stiffness at all ranges. Night pain, both have night pain but frozen shoulder often more severe. Onset, impingement gradual from overuse, frozen shoulder often spontaneous or post-injury. However, they can coexist, chronic impingement can lead to secondary frozen shoulder from disuse. Accurate diagnosis requires examination by shoulder specialist.
Subacromial bursitis is inflammation and thickening of the bursa (fluid-filled cushion) in the subacromial space. Shoulder bursitis and impingement syndrome often occur together, in fact, bursitis is usually part of impingement syndrome. The relationship: (1) Impingement compresses the bursa causing inflammation (bursitis). (2) The inflamed swollen bursa takes up space, worsening the impingement. (3) This creates a vicious cycle. Treatment is essentially the same: rest, NSAIDs, physical therapy, corticosteroid injections (very effective for bursitis), surgical bursa excision if conservative treatment fails. So while technically different anatomically, shoulder bursitis and impingement are almost always treated together as one condition.
Sleeping after rotator cuff surgery requires a reclined position for 4-6 weeks a recliner is ideal, otherwise use a wedge pillow at 45 degrees. Lying flat increases pressure on the repair and pain. Ice every 2 hours for 20 minutes significantly reduces swelling during early recovery.
Related Conditions & Procedures
Related Conditions
Rotator Cuff Tear Treatment, chronic impingement leads to tears· Frozen Shoulder Treatment, can develop from chronic impingement. · Shoulder Instability Treatment, different pathology· Bicep Tendonitis Treatment, often coexists· Shoulder Treatment Dubai, comprehensive hub
Related Procedures
Subacromial Decompression Surgery, when conservative fails· Rotator Cuff Repair Surgery, if tear present· Shoulder Arthroscopy, technique overview
Take control of your health, mobility, and quality of life.
Your First Step Toward a Stronger Tomorrow Starts Now:
Book your personal consultation with Dr. Usama Saleh today and begin your journey to a better you.
Thank you — your message was sent.
