
ACL & Meniscus Tear Treatment in Dubai | Dr. Usama Saleh
The pop of an ACL tear. The catching pain of a meniscal injury that interrupts every training session. These are two of the most common and consequential knee injuries in Dubai’s active population , and two conditions where accurate diagnosis and the right surgical decision make a career-defining difference. Dr. Usama Saleh, a fellowship-trained orthopedic knee surgeon with 23+ years of experience, provides expert ACL and meniscus tear assessment and treatment at Medcare Orthopaedics & Spine Hospital (MOSH), Sheikh Zayed Road, Dubai. Whether you need arthroscopic meniscal repair, ACL reconstruction, or confirmation that conservative management is the right call for your specific injury , your recovery starts with an accurate diagnosis and a plan built around your sport, your age, and your timeline.
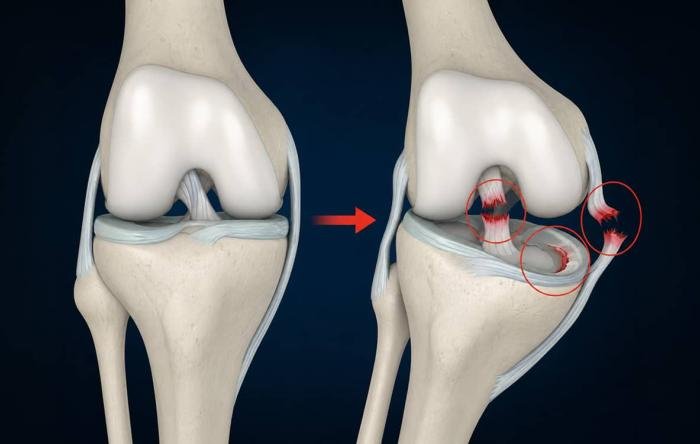
What Are ACL & Meniscus Tears?
Anterior Cruciate Ligament
The ACL runs diagonally through the knee's center, connecting femur to tibia. It acts as the primary restraint against rotational instability and anterior translation. Ruptures happen under intense rotational or hyperextension force. Complete tears cannot heal spontaneously; the ligament retracts, rendering the joint chronically unstable without reconstruction.

The Menisci Structure
Two C-shaped wedges of fibrocartilage serving as critical shock absorbers, distributing up to 70% of compressive loads. Tears range from avascular inner zones (irreparable splits) to peripheral vascular outer zones (surgically repairable).
Of acute ACL tears present a co-occurring meniscal rupture at exploration. Rotational forces simultaneously compromise both structures, altering rehabilitation pathways.
Types of ACL & Meniscus Tears Treated by Dr. Usama
Complete ACL Tear
Full-thickness ACL disruption, the hallmark audible pop, immediate hemarthrosis, and gross rotational instability. ACL reconstruction is recommended for active patients wanting to return to pivoting sports. Cannot heal spontaneously.
Partial ACL Tear
Partial fiber disruption: the ligament remains in continuity but is stretched and weakened. May allow return to sport with rehabilitation in less active individuals. High-demand athletes with clinical instability may still require reconstruction.
Medial Meniscal Tear
The most common meniscal injury is the larger, C-shaped medial meniscus. Posterior horn medial meniscal tears are most frequent. Ranges from repairable peripheral flap tears to complex degenerative tears requiring partial meniscectomy.
Lateral Meniscal Tear
Most commonly associated with acute ACL tears, the lateral compartment absorbs the pivot-shift forces that rupture the ACL. Lateral tears are more frequently repairable due to better blood supply.
Bucket-Handle Meniscal Tear
A longitudinal tear with central displacement into the joint space, mechanically blocking full knee extension. Results in a locked knee requiring urgent arthroscopic reduction and repair or meniscectomy. A surgical emergency.
Combined ACL + Meniscus Tear
The most frequent serious knee injury combination is an ACL rupture with a concurrent meniscal tear. Requires comprehensive MRI assessment and combined arthroscopic surgery: ACL reconstruction plus meniscal repair or meniscectomy in a single procedure.
Symptoms of ACL Tears vs. Meniscus Tears
Scroll or hover to freeze. Accurate differentiation guides urgent assessment decisions.
The Audible Pop
A loud pop or crack felt or heard at the moment of injury, the hallmark symptom in approximately 70% of complete ACL tears.
Rapid Swelling
Immediate and rapid knee swelling within 1-2 hours of injury, haemarthrosis (blood in the joint) indicating major structural damage.
Functional Failure
Immediate inability to continue sport; the knee feels unable to hold weight or absorb the forces of athletic movement.
Giving Way
Persistent sense of instability, buckling, or giving way during weight-bearing, particularly during pivoting, cutting, or descending stairs.
Restricted Motion
Difficulty fully straightening or bending the knee in the acute phase due to hemarthrosis and muscle guarding.
The Audible Pop
A loud pop or crack felt or heard at the moment of injury, the hallmark symptom in approximately 70% of complete ACL tears.
Rapid Swelling
Immediate and rapid knee swelling within 1-2 hours of injury, haemarthrosis (blood in the joint) indicating major structural damage.
Functional Failure
Immediate inability to continue sport; the knee feels unable to hold weight or absorb the forces of athletic movement.
Giving Way
Persistent sense of instability, buckling, or giving way during weight-bearing, particularly during pivoting, cutting, or descending stairs.
Restricted Motion
Difficulty fully straightening or bending the knee in the acute phase due to hemarthrosis and muscle guarding.
Joint Line Pain
Pain along the inner (medial) or outer (lateral) knee joint line, localized to the specific meniscus, often pinpoint-accurate with direct palpation.
Delayed Swelling
Swelling that develops more gradually than ACL tears, typically appearing 24-48 hours after injury.
Mechanical Catching
A clicking, catching, or locking sensation during knee movement, indicating a displaced meniscal fragment.
True Knee Locking
Full locking of the knee with inability to fully straighten indicates a bucket-handle tear requiring urgent surgical assessment.
Loading Pain
Pain worsening with pivoting, squatting, or climbing stairs, activities that compress and load the menisci.
Fluctuating Distress
Pain that fluctuates, improves with rest but recurs with return to loading activities.
Joint Line Pain
Pain along the inner (medial) or outer (lateral) knee joint line, localized to the specific meniscus, often pinpoint-accurate with direct palpation.
Delayed Swelling
Swelling that develops more gradually than ACL tears, typically appearing 24-48 hours after injury.
Mechanical Catching
A clicking, catching, or locking sensation during knee movement, indicating a displaced meniscal fragment.
True Knee Locking
Full locking of the knee with inability to fully straighten indicates a bucket-handle tear requiring urgent surgical assessment.
Loading Pain
Pain worsening with pivoting, squatting, or climbing stairs, activities that compress and load the menisci.
Fluctuating Distress
Pain that fluctuates, improves with rest but recurs with return to loading activities.
What Causes ACL & Meniscus Tears?
Understanding injury mechanisms and predisposing risk factors.
ACL Injury Mechanisms
Non-Contact Pivoting
Sudden deceleration combined with a rotational force while the foot is planted. Most common in football, basketball, rugby, and padel.
Hyperextension Force
The knee is forced beyond its normal extension limit during landing or sharp contact injuries, causing direct ligament failure.
Direct Contact
Valgus or varus force applied directly from an external tackle or collision, frequently seen in contact sports.
Meniscal Tear Mechanisms
Acute Athletic Tears
Sudden rotation while the knee is flexed and weight-bearing; the fibrocartilage gets trapped between the femur and tibia during twisting movements.
Degenerative Tears (Over 40)
Can occur from minimal force like a simple squat, rising from a chair, or an uneven step, reflecting underlying cartilage degeneration.
Key Risk Factors
Anatomical, physiological, and environmental predispositions.
Female Athlete Risk
2-4x higher risk due to hormonal, anatomical, and neuromuscular parameters.
Previous Rupture
Prior ACL injury (contralateral or ipsilateral) remains the highest individual re-rupture factor.
High-Demand Sports
Rapid deceleration, cutting, and pivoting: football, rugby, basketball, padel, skiing, and netball.
Age-Related Shift
Age over 35 shifts susceptibility toward progressive degenerative meniscal pathology.
ACL Insufficiency
Unstable joints accelerate meniscal wear, adding an estimated 10% new tear risk per year.
Anatomic Predisposition
A narrow intercondylar notch presents an inherent structural risk for mechanical impingement.
How Dr. Usama Diagnoses ACL & Meniscus Tears
Accurate diagnosis combines validated clinical examination with MRI imaging. Clinical examination alone misses approximately 20-30% of meniscal tears; MRI is essential for surgical planning.
Clinical Examination
ACL Assessment: Lachman test is the most sensitive (84-87%), performed at 30° flexion to assess endpoint quality, alongside Anterior drawer and Pivot shift tests (near 100% specific for rotational instability).
Meniscus Assessment: McMurray test (tibial rotation during flexion-extension), Apley compression, and Thessaly tests. Joint line palpation isolates medial vs. lateral pathology with high clinical accuracy.
Diagnostic Imaging
MRI (Gold Standard): 86-95% sensitive for complete ACL tears and 77-93% for meniscal tears. Identifies bone bruising and chondral status. Dr. Usama reviews the MRI with each patient at consultation.
Weight-Bearing X-rays: Exclude tibial spine avulsion fractures, patella fractures, osteochondral defects, and pre-existing osteoarthritis which impacts surgical choices.











Treatment Options for ACL & Meniscus Tears
Treatment is determined by tear type, patient age, activity demands, and MRI findings.
Conservative Treatment (Selected Cases)
Physiotherapy & Rehabilitation
First-line for partial ACL tears in less active patients over 40, degenerative meniscal tears in patients over 50 with low activity demands, and inner-zone meniscal tears. Targets quadriceps/hamstring strengthening. Effective in 60-75% of selected candidates.
PRP Injection Therapy
Used selectively as an adjunct to rehabilitation for partial ACL tears and degenerative meniscal pathology to stimulate biological repair.
Surgical Treatment (Arthroscopic Approach)
ACL Reconstruction
Definitive treatment for complete ACL tears in active patients. Utilizing autografts (hamstring tendon for recreational athletes; patellar tendon for elite athletes) or allografts with anatomic tunnel placement.
Arthroscopic Meniscal Repair
Preferred over meniscectomy for vascular outer zone tears. Sutures approximate torn edges with a 70-85% healing rate. Tissue preservation significantly reduces long-term OA risk.
Partial Meniscectomy
For non-repairable inner-zone or complex degenerative tears. Minimally damaged tissue is removed arthroscopically. Same-day procedure (45-60 min). Full return to sport in 6-8 weeks.
Combined ACL + Meniscal Surgery
Both injuries addressed in a single procedure. Avoids a second operation. Complete recovery time takes typically 9-12 months for competitive sports, governed by the ACL recovery protocol.




When Should You See a Doctor for a Knee Injury in Dubai?
The most important factor determining ACL and meniscal tear outcome is timeliness of accurate diagnosis. Earlier specialist assessment produces consistently better outcomes.
Dr. Usama Saleh
Medcare MOSH, Sheikh Zayed Road, Dubai
Locked Knee & Traumatic Dislocation
Your knee is completely locked, and you cannot fully straighten it (displaced bucket-handle meniscal tear). Or you have had a high-energy traumatic knee dislocation which can damage the ACL, PCL, and critically, the popliteal artery. Requires urgent vascular assessment.
Rapid Swelling & Gross Instability
Your knee swelled rapidly within 1-2 hours after a sports injury (hemarthrosis pattern indicating an ACL tear). Or the knee feels unstable, buckles, and gives way during weight-bearing since the injury, threatening further meniscal damage.
Persistent Pain & Missed Sprains
Joint line pain has persisted for more than 2-4 weeks following a twisting or squatting injury. Also essential if you have been diagnosed with a knee sprain but are not recovering in the expected timeframe (commonly missed ACL/meniscal tears).
Seasonal Clarity & Dubai Specialist Care
Active athletes needing clarity on whether an injury requires surgery before season planning. Dr. Usama provides same-day consultation, MRI reviews, and clear diagnoses for acute knee injuries in Dubai.
Locked Knee & Traumatic Dislocation
Your knee is completely locked, and you cannot fully straighten it (displaced bucket-handle meniscal tear). Or you have had a high-energy traumatic knee dislocation which can damage the ACL, PCL, and critically, the popliteal artery. Requires urgent vascular assessment.
Rapid Swelling & Gross Instability
Your knee swelled rapidly within 1-2 hours after a sports injury (hemarthrosis pattern indicating an ACL tear). Or the knee feels unstable, buckles, and gives way during weight-bearing since the injury, threatening further meniscal damage.
Persistent Pain & Missed Sprains
Joint line pain has persisted for more than 2-4 weeks following a twisting or squatting injury. Also essential if you have been diagnosed with a knee sprain but are not recovering in the expected timeframe (commonly missed ACL/meniscal tears).
Seasonal Clarity & Dubai Specialist Care
Active athletes needing clarity on whether an injury requires surgery before season planning. Dr. Usama provides same-day consultation, MRI reviews, and clear diagnoses for acute knee injuries in Dubai.
Exercises for ACL & Meniscus Tears: What Is Safe and When
Pre-Surgical Rehabilitation (Pre-Hab)
Six or more weeks of structured pre-hab before ACL reconstruction significantly improve postoperative outcomes.
Quadriceps Sets
Sit on the floor, affected leg straight. Tighten the quadriceps by pressing the back of the knee toward the floor, hold for 5 seconds, and release.
Straight Leg Raises
Lie on your back, unaffected knee bent, and affected leg straight. Tighten the quadriceps, raise the affected leg to the height of the bent knee, hold for 3 seconds, and lower slowly.
Heel Slides
Lie on your back. Slowly slide the heel toward your buttocks, bending the knee to a comfortable range, then straighten slowly. Restores range of motion without rotational loading.
Calf Raises
Stand holding a surface for balance. Rise onto the balls of both feet, hold for 3 seconds, and lower slowly. Prevents calf atrophy and maintains dynamic stability.
Short Arc Quads
Lie on your back with a rolled towel under the knee at 30 degrees of flexion. Straighten the knee fully against gravity, hold for 3 seconds, and lower slowly. Critical for terminal extension.
Meniscal Tears Conservative Management
Tailored for non-locked knees to gently restore flexibility and functional quadriceps capability.
Heel-to-Buttock Stretch (Prone)
Lie face down. Slowly bend the knee toward the buttocks to a comfortable range. Hold for 30 seconds. Gently restores knee flexion range lost through swelling.
Step-Ups (Low Step, 10-15 cm)
Step up and down slowly with control. Strengthens quadriceps and glutes in a functional pattern without loading the meniscus in deep flexion.
Prohibited Movements & Clinical Safety
Do not perform deep squats, lunges, or any exercise involving deep knee flexion past 90 degrees with a confirmed meniscal tear; this loads the posterior horn directly and can worsen the tear. Avoid twisting and pivoting movements. All exercises should be performed pain-free.
How ACL Reconstruction & Meniscal Surgery Are Performed, Step by Step
A meticulously timed arthroscopic approach engineered for joint stability and structural preservation.
1. Anesthesia & Positioning
General anesthesia combined with a femoral nerve block providing 12-18 hours of post-operative pain control. Patient positioned supine with a stable leg holder; the surgical site is prepared and sterilized.
2. Arthroscopic Assessment
2-3 small 5-10 mm portals are created. An HD arthroscope provides magnified visualization of the entire knee interior. Both menisci, articular cartilage, and the ACL are systematically assessed, confirming MRI findings.
3. Meniscal Treatment First
Meniscal repair (suture passage and fixation for peripheral tears) or partial meniscectomy is performed before ACL reconstruction, allowing free knee movement during graft passage without impingement.
4. Graft Harvest
Hamstring autograft: gracilis & semitendinosus harvested via a 2-3 cm incision (prepared as a 4-strand graft, 8-10 mm diameter). Patellar tendon autograft: central third strip with bone plugs via a 3-4 cm incision, preferred for elite athletes.
5. Tunnel Drilling & Graft Fixation
Tibial and femoral bone tunnels are drilled at native anatomic attachment sites to restore translational and rotational stability. Grafts are passed and secured with interference screws or cortical buttons.
6. Final Inspection & Closure
Full ROM testing confirms graft position and absence of roof impingement. Portals closed with 1-2 absorbable sutures. Hinged knee brace applied for same-day discharge from Medcare MOSH.
Surgical Duration & Facility Timeline
| Procedure Type | Surgical Duration | Total Facility Time (MOSH) |
|---|---|---|
| ACL Reconstruction Alone | 75-90 minutes | 4-6 Hours Including pre-op & recovery |
| ACL + Meniscal Repair | 90-120 minutes | |
| ACL + Meniscectomy | 75-100 minutes | |
| Meniscal Repair Only | 60-90 minutes | |
| Partial Meniscectomy Only | 45-60 minutes |
Recovery After ACL & Meniscus Tear Surgery in Dubai
The standardized rehabilitation framework engineered at Medcare MOSH Dubai to safely restore athletic capabilities.
Phase 1: Protection
Hinged knee brace locked at 0-90°. Crutches for partial weight-bearing (0-4 wks for ACL, 0-6 wks for meniscal repair). Focus on ice, elevation, oral analgesia, quadriceps activation, and swelling management.
Phase 2: Restoring Function
Full weight-bearing commenced. Brace discontinued. Active ROM restoration. Pool-based rehab from weeks 6-8. Progressive quadriceps and hamstring strengthening. Desk work return: 1-4 wks.
Phase 3: Strengthening
Progressive resistance training (leg press, squats, step-ups, leg curls). Proprioceptive and neuromuscular control training (single-leg balance, perturbation training). Light jogging starts weeks 14-16.
Phase 4: Return to Sport
Full competitive pivoting sport return 9-12 months. Clearance criteria: quad/hamstring strength >90% of contralateral leg; limb symmetry index on hop testing >90%;Passed sport agility and psychological readiness.
Clinical Return-to-Activity Timeline Matrix
| Injury Type | Desk Work | Driving | Sport Training | Competition Return |
|---|---|---|---|---|
| ACL Reconstruction | 1-2 Weeks | 6-8 Weeks | 8-10 Months | 9-12 Months |
| ACL + Meniscal Repair | 1-2 Weeks | 6-8 Weeks | 9-11 Months | 10-12 Months |
| Meniscal Repair Only | 1-2 Weeks | 4-6 Weeks | 4-5 Months | 4-6 Months |
| Partial Meniscectomy | 1 Week | 2-3 Weeks | 4-6 Weeks | 6-8 Weeks |
Preparing for Your ACL or Meniscal Tear Consultation & Surgery
Comprehensive preparation significantly reduces recovery timelines and enhances clinical outcomes.
Consultation Prep
Bring all previous imaging (MRIs, X-rays) and reports. Prepare an injury timeline: date, mechanism, presence of a pop, timing of swelling, and previous treatments.
Pre-Hab Period
Complete 4-6 weeks of structured pre-hab physiotherapy. Evidence shows 6+ weeks of preoperative rehab improves ACL reconstruction outcomes and accelerates return to sport.
2-4 Weeks Before
STOP SMOKING (doubles infection risk and impairs healing). Stop blood thinners and NSAIDs per clinical instructions. Arrange home preparation, crutches, and brace.
Day of Surgery
Arrive 1.5-2 hours early. Nil by mouth from midnight. Bring photo ID and insurance card. A designated driver is mandatory for discharge from Medcare MOSH.
Consultation Prep
Bring all previous imaging (MRIs, X-rays) and reports. Prepare an injury timeline: date, mechanism, presence of a pop, timing of swelling, and previous treatments.
Pre-Hab Period
Complete 4-6 weeks of structured pre-hab physiotherapy. Evidence shows 6+ weeks of preoperative rehab improves ACL reconstruction outcomes and accelerates return to sport.
2-4 Weeks Before
STOP SMOKING (doubles infection risk and impairs healing). Stop blood thinners and NSAIDs per clinical instructions. Arrange home preparation, crutches, and brace.
Day of Surgery
Arrive 1.5-2 hours early. Nil by mouth from midnight. Bring photo ID and insurance card. A designated driver is mandatory for discharge from Medcare MOSH.
Risks & Expected Outcomes of ACL & Meniscal Tear Treatment
Complete transparency about risks serves patients better than reassurance that minimizes genuine considerations.
Surgical Risks & Complications
General Surgical Risks
- Infection: <1% with arthroscopic technique and prophylactic antibiotics.
- DVT / PE: <1% with early mobilization protocol.
- Anaesthesia Complications: <1%, minimized by pre-operative assessment.
ACL-Specific Risks
- Graft Failure (Re-rupture): 5-15% depending on graft type, age, and rehab compliance. Risk is significantly higher before 9 months.
- Quadriceps Strength Deficit: 10-20% vs contralateral leg at 6 months, resolved with full 9-12 month rehab.
- Knee Stiffness (Arthrofibrosis): 5-10%, prevented by early physiotherapy initiation.
Meniscal-Specific Risks
- Repair Re-tear: 10-20% for peripheral tears, higher for complex patterns.
- Persistent Pain: 5-10% after partial meniscectomy.
Expected Success Rates
ACL Reconstruction
85-90%Return to pre-injury sport level at 9-12 months. 90-95% graft survival at 5 years with appropriate rehabilitation protocols.
Meniscal Repair
70-85%Healing rate for peripheral tears. 85-90% pain improvement with an 85% return to sport achieved at 4-6 months.
Partial Meniscectomy
85-90%Patient satisfaction rate. Return to sport in 6-8 weeks. Note: Long-term OA risk is increased versus surgical repair.
What Happens if an ACL or Meniscus Tear Is Left Untreated?
Without appropriate management, both conditions follow a predictable trajectory of progressive structural deterioration.
Untreated ACL Tear Consequences
Recurrent Giving-Way
Each episode of instability applies damaging shear forces directly to the medial meniscus, articular cartilage, and secondary knee stabilisers during athletic movements.
Secondary Meniscal Tears
ACL-deficient knees develop new meniscal tears at an estimated rate of 10% per year without reconstruction, significantly raising future surgical complexity.
Early-Onset Knee Osteoarthritis
Combined instability, progressive meniscal loss, and structural cartilage damage lead to premature knee OA at higher rates if reconstruction is delayed.
Untreated Meniscal Tear Consequences
Progressive Cartilage Wear
A damaged meniscus exposes cartilage to 3x to 5x normal contact stress, accelerating surface wear proportional to the amount of tissue damaged.
Knee OA Acceleration
Total meniscectomy is linked with a 70% radiographic OA incidence within 15 years. Partial meniscectomy also increases risk, highlighting Dr. Usama's repair-first philosophy.
Chronic Functional Limitation
Untreated bucket-handle tears cause persistent pain, swelling, and permanent inability to achieve full extension, severely impacting gait and occupational function.
Why Choose Dr. Usama Saleh for ACL & Meniscal Tear Treatment in Dubai?
Fellowship-Trained Knee Specialist
Advanced fellowship training at the University of Toronto provided deep subspecialty expertise in complex ACL reconstruction techniques, advanced meniscal repair strategies, and multi-ligament injury management beyond standard orthopedic qualifications.
Graft Selection Expertise
Hamstring autograft: faster donor-site recovery, preferred for recreational athletes. Patellar tendon autograft: bone-to-bone fixation with rapid biological incorporation, engineered for elite athletes needing maximal early stability.
Meniscal Preservation Philosophy
Dr. Usama prioritizes meniscal repair over removal wherever tissue quality allows. Preserving native cartilage produces significantly better long-term outcomes and reduces osteoarthritis risk, even when a meniscectomy would be technically simpler.
23+ Years of High-Volume Experience
Two decades of dedicated orthopedic knee surgery in Dubai covering professional football, rugby, basketball, padel, and skiing injuries across all age groups, from adolescent growth plates to master-level sports competitors.
Integrated ACL Rehabilitation
Dr. Usama works in seamless, direct collaboration with specialist sports physiotherapists at Medcare MOSH. This ensures your post-operative recovery protocol is tightly coordinated, eliminating communication gaps between surgeon and therapy team.
International Research & Teaching Authority
An active AO Trauma faculty member, published peer-reviewed manuscript author, and international conference presenter. Your knee care is directly guided by global evidence-based orthopedic innovations.














Real Patients, Real Recovery: ACL & Meniscus Success Stories
Discover firsthand accounts of recovery, joint stability, and return to competitive sports in Dubai.
"I ruptured my ACL playing football in Dubai. Dr. Usama performed ACL reconstruction and designed my rehabilitation. I was back playing competitive football at 10 months."
"I had a complex meniscal tear with a bucket-handle component locking my knee. Dr. Usama performed same-day arthroscopic repair, prioritising preserving tissue. Back running at 5 months."
"Combined ACL and medial meniscal tear from a skiing accident. Dr. Usama addressed both in the same operation, explained every step clearly. Back skiing at 12 months."
"As a padel player, knee stability is everything. Dr. Usama diagnosed my partial ACL tear and managed it conservatively with PRP and targeted physio. My knee feels incredibly stable now."
"Dr. Usama is the most transparent surgeon in Dubai. He reviewed my knee MRI, explained the lateral meniscus split, and performed a perfect arthroscopic repair. Highly recommended."
"Severe joint line pain for months was misdiagnosed as a sprain elsewhere. Dr. Usama immediately identified the posterior horn meniscus tear. Partial meniscectomy solved it. Pain-free in 6 weeks."
"Highly professional team at Medcare MOSH. Dr. Usama repaired my torn ACL using a patellar tendon graft. The early stability is amazing, and my recovery is ahead of schedule."
"I had chronic knee giving-way episodes due to an old untreated ACL injury. Dr. Usama reconstructed the ligament and saved my cartilage from further tearing. Absolute expert."
"I ruptured my ACL playing football in Dubai. Dr. Usama performed ACL reconstruction and designed my rehabilitation. I was back playing competitive football at 10 months."
"I had a complex meniscal tear with a bucket-handle component locking my knee. Dr. Usama performed same-day arthroscopic repair, prioritising preserving tissue. Back running at 5 months."
"Combined ACL and medial meniscal tear from a skiing accident. Dr. Usama addressed both in the same operation, explained every step clearly. Back skiing at 12 months."
"As a padel player, knee stability is everything. Dr. Usama diagnosed my partial ACL tear and managed it conservatively with PRP and targeted physio. My knee feels incredibly stable now."
"Dr. Usama is the most transparent surgeon in Dubai. He reviewed my knee MRI, explained the lateral meniscus split, and performed a perfect arthroscopic repair. Highly recommended."
"Severe joint line pain for months was misdiagnosed as a sprain elsewhere. Dr. Usama immediately identified the posterior horn meniscus tear. Partial meniscectomy solved it. Pain-free in 6 weeks."
"Highly professional team at Medcare MOSH. Dr. Usama repaired my torn ACL using a patellar tendon graft. The early stability is amazing, and my recovery is ahead of schedule."
"I had chronic knee giving-way episodes due to an old untreated ACL injury. Dr. Usama reconstructed the ligament and saved my cartilage from further tearing. Absolute expert."
"My teenage son suffered an ACL avulsion fracture. Dr. Usama explained everything to us clearly and performed a highly successful arthroscopic fixation. His recovery has been fantastic."
"I had a degenerative meniscus tear at age 48. Dr. Usama guided me through a structured 6-week non-surgical pre-hab program instead of rushing into surgery. The results are flawless."
"After a bad tackle in rugby, my knee swelled rapidly with extreme pain. Dr. Usama's urgent assessment and subsequent multi-ligament surgery saved my seasonal training program. Infinite thanks."
"Dr. Usama prioritised repairing my lateral meniscus instead of a quick meniscectomy. Preserving the cartilage protects my knee from future arthritis. A truly ethical and master surgeon."
"The same-day arthroscopic surgery at Medcare MOSH was exceptionally smooth. Dr. Usama and the femoral nerve block made post-op pain management incredibly easy. Outstanding care."
"I flew from Oman specifically to see Dr. Usama for a re-ruptured ACL. His anatomic tunnel reconstruction technique fixed my chronic buckling joint. The best knee specialist near me."
"I had severe knee locking from a complex bucket-handle meniscus tear. Dr. Usama adjusted his schedule for an urgent arthroscopic reduction. He completely saved my joint functionality."
"Six weeks of pre-hab recommended by Dr. Usama made a world of difference. I entered ACL surgery strong and my quad strength post-reconstruction returned faster than expected."
"My teenage son suffered an ACL avulsion fracture. Dr. Usama explained everything to us clearly and performed a highly successful arthroscopic fixation. His recovery has been fantastic."
"I had a degenerative meniscus tear at age 48. Dr. Usama guided me through a structured 6-week non-surgical pre-hab program instead of rushing into surgery. The results are flawless."
"After a bad tackle in rugby, my knee swelled rapidly with extreme pain. Dr. Usama's urgent assessment and subsequent multi-ligament surgery saved my seasonal training program. Infinite thanks."
"Dr. Usama prioritised repairing my lateral meniscus instead of a quick meniscectomy. Preserving the cartilage protects my knee from future arthritis. A truly ethical and master surgeon."
"The same-day arthroscopic surgery at Medcare MOSH was exceptionally smooth. Dr. Usama and the femoral nerve block made post-op pain management incredibly easy. Outstanding care."
"I flew from Oman specifically to see Dr. Usama for a re-ruptured ACL. His anatomic tunnel reconstruction technique fixed my chronic buckling joint. The best knee specialist near me."
"I had severe knee locking from a complex bucket-handle meniscus tear. Dr. Usama adjusted his schedule for an urgent arthroscopic reduction. He completely saved my joint functionality."
"Six weeks of pre-hab recommended by Dr. Usama made a world of difference. I entered ACL surgery strong and my quad strength post-reconstruction returned faster than expected."
Why Choose Dr. Usama
For Frozen Shoulder Treatment In Dubai
Best Shoulder Doctor Dubai — Fellowship-Trained
23+ Years as Dubai's Shoulder Specialist Doctor
Expert in How to Treat Rotator Cuff Tear — All Options
Honest — Surgery Only When Truly Needed
Frequently asked questions
Need something cleared up? Here are our most frequently asked questions.
An ACL tear is damage to the anterior cruciate ligament, a ligament inside the knee providing stability against rotational and anterior forces. It tears under pivoting or hyperextension mechanisms, causes immediate instability and rapid swelling, and requires reconstruction with a graft for active patients. A meniscal tear is damage to the fibrocartilage shock absorbers (medial or lateral meniscus) sitting between the femur and tibia. Meniscal tears cause joint line pain, clicking or catching, and often delayed swelling. Both are diagnosed by MRI and treated arthroscopically but have completely different surgical approaches. ACL requires full reconstruction with a graft, while meniscal tears may be repaired or partially removed.
ACL tear indicators: a loud pop at injury, rapid swelling within 1-2 hours, immediate inability to continue sports, and persistent giving way or instability. Meniscal tear indicators: pain along the inner or outer knee joint line, swelling developing 24-48 hours post-injury, clicking or catching sensations, pain with squatting or pivoting. Only an MRI interpreted by an experienced orthopedic knee surgeon accurately distinguishes and grades these injuries; a clinical examination alone misses approximately 20-30% of meniscal tears.
It depends on the specific tear type and location. Meniscal tears in the vascular outer zone (peripheral 25-30%) have healing potential with conservative management in appropriate patients , older patients with lower activity demands, stable knees, and no locking. Tears in the avascular inner zone (inner 70-75%) cannot heal regardless of treatment. Complete surgical repair is required for locked knees (bucket-handle tears) and tears in active patients seeking return to pivoting sport. Dr. Usama assesses each tear individually on location, pattern, tissue quality, and patient demands.
Most patients can walk after the initial swelling settles; walking on flat surfaces does not significantly load the ACL. However, activities requiring pivoting, cutting, quick directional changes, or running in place place substantial rotational demands on the ACL-deficient knee, causing giving-way episodes that damage the menisci and cartilage with every episode. The ability to walk is not a reliable indicator of injury severity. An ACL-deficient knee functioning adequately for walking may be destroying itself during return to sport.
ACL reconstruction recovery follows a 9-12 month protocol for a full return to competitive pivoting sports. This timeline applies equally to patients from Dubai, Abu Dhabi, and across the UAE who undergo surgery at Medcare MOSH. Key milestones: weeks 1-2 desk work; weeks 6-8 driving (non-dominant leg); weeks 12-16 jogging commences; months 6-9 sport-specific training; months 9-12 clearance based on objective strength and functional testing criteria rather than calendar dates. Meniscal repair performed at the same time may extend sport return by 1-2 months due to healing requirements.
No, ACL reconstruction is not universally required. Appropriate non-surgical management is indicated for partial ACL tears with clinical stability and low activity demands; complete tears in patients over 50-55 with predominantly walking and recreational demands; and patients with significant comorbidities. The decision is based on patient age, activity demands, clinical stability, MRI findings, and shared decision-making. Dr. Usama presents both surgical and conservative expected outcomes honestly.
Meniscus tear recovery time depends on treatment type: Conservative management: meniscus tear recovery time is 6-12 weeks for minor tears with adequate improvement. Partial meniscectomy: meniscus tear recovery time is 2-4 weeks to light activity and 6-8 weeks to full unrestricted sport, the fastest recovery option. Arthroscopic meniscal repair: meniscus tear recovery time is 4-6 months to return to contact sports; the sutured tissue requires biological healing time. Dr. Usama provides personalized meniscus tear recovery timelines at consultations based on your tear type, procedure, and sport demands.
Book Your ACL or Meniscal Tear Consultation in Dubai
Whether you need confirmation of an ACL diagnosis, a second opinion on surgical necessity, or expert management, Dr. Usama Saleh provides the specialist assessment that gets the diagnosis right.
Accepted Health Insurance Networks
ACL & Meniscus Tear Treatment in Dubai, Serving Athletes Across the UAE
ACL tears and meniscal injuries are the most frequent serious knee conditions in Dubai's active population. From the football pitches of Jumeirah to the padel courts of JBR and Business Bay, early specialist assessment produces consistently better outcomes.
Dr. Usama sees patients from across Dubai's communities as well as regional athletes. If you are searching for an ACL specialist near you, our team can confirm same-day or urgent appointment availability at Medcare MOSH on Sheikh Zayed Road.
Clinical Location Registry
Take control of your health, mobility, and quality of life.
Your First Step Toward a Stronger Tomorrow Starts Now:
Book your personal consultation with Dr. Usama Saleh today and begin your journey to a better you.
Thank you — your message was sent.
