Understanding
Frozen Shoulder
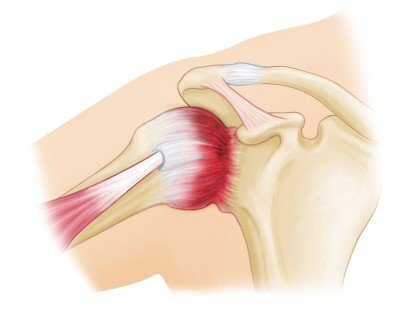
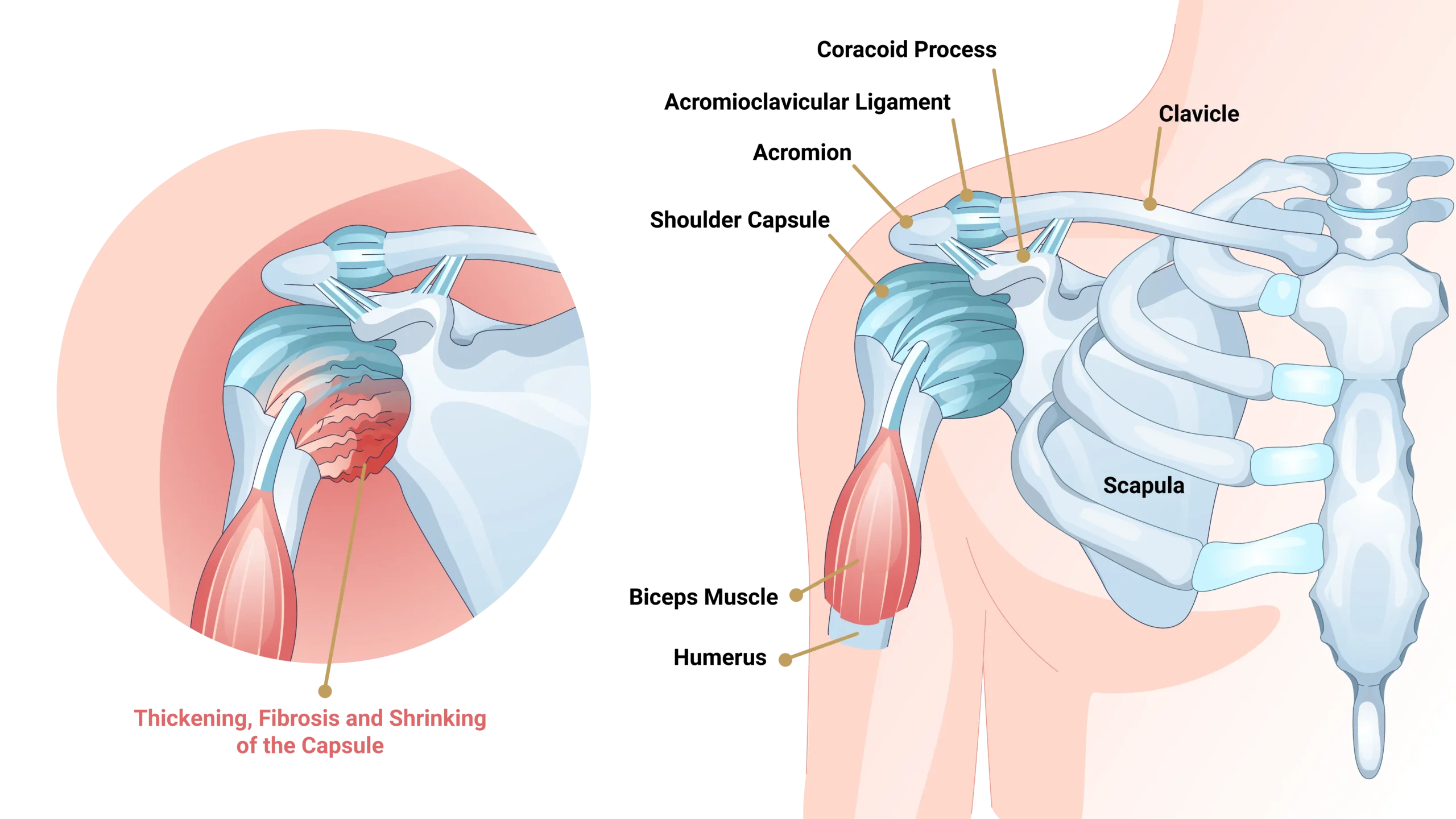
Frozen shoulder, clinically termed adhesive capsulitis, is a highly restrictive pathology targeting the connective tissue envelope of the joint.
The condition occurs when the shoulder joint capsule becomes profoundly inflamed, thickened, and contracted. This global capsular tightening severely restricts both active movement (you moving your arm) and passive movement (someone else moving your arm).
The Unique Diagnostic Indicator:
Unlike most subacromial or rotator cuff conditions where passive motion remains intact, frozen shoulder uniquely limits movement in all operational planes with a distinct, characteristic ‘hard stop’ mechanical block upon clinical testing.
Diagnosis Of
Frozen Shoulder
Frozen shoulder diagnosis is primarily clinical. Dr. Usama maps the characteristic restriction patterns to isolate capsular pathology from other joint conditions accurately.
Board certified in orthopedics surgery
Clinical Examination
Testing reveals severe range of motion restriction in all directions, notably forward flexion, abduction, and external rotation (the most limited plane). A key differentiator is that both active and passive ROM are limited, tracking a strict 'capsular pattern' with a smooth, solid 'hard stop' at end range, completely free of crepitus or grinding.
Imaging Studies
X-rays & MRI: X-rays typically return normal parameters, serving primarily to rule out joint arthritis or calcific tendinitis. MRI can visualize a thickened joint capsule and decreased joint volume metrics but is generally not required for definitive confirmation.
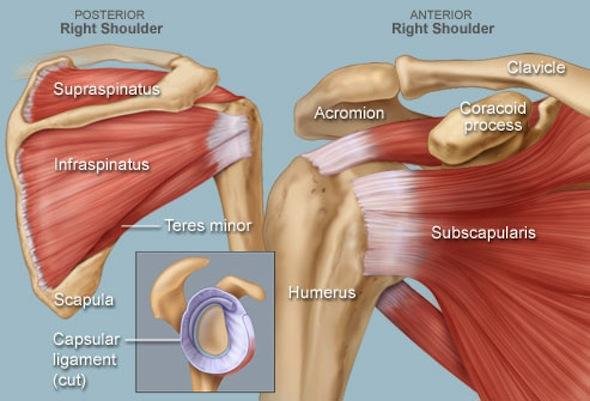
Ultrasound Tracking: May show explicit coracohumeral ligament thickening. Imaging is deployed mainly as a protective check to rule out secondary rotator cuff tears if the diagnosis remains unclear.










Exercises & Physical Therapy
Frozen shoulder exercises are the absolute cornerstone of non-surgical clinical treatment. Consistent daily stretching is essential to systematically expand contracted capsular tissue envelopes.
Targeted Clinical Protocols (Infinity Loop)
Pendulum Exercises
Lean forward letting the affected arm hang freely. Initiate gentle circular motions utilizing gravity-assisted stretching metrics. Safe and highly indicated across all chronological staging fields.
Wall Walks Stretch
Face a wall directly, walking your fingers up progressively to capture incremental forward flexion stretch. Hold the peak terminal point for 30 seconds to accurately mark structural progress over weeks.
External Rotation Stretch
Utilize doorway parameters or stick-assisted mechanics. Adhesive capsulitis exercises must include external rotation, as it targets the most structurally restricted joint motion field. Hold for 30-60 seconds.
Overhead Pulley Care
Deploy an overhead pulley system, using the healthy opposite arm to gently assist and guide the affected arm overhead. Provides a highly controlled, progressive, non-traumatic joint envelope stretch.
Pendulum Exercises
Lean forward letting the affected arm hang freely. Initiate gentle circular motions utilizing gravity-assisted stretching metrics. Safe and highly indicated across all chronological staging fields.
Wall Walks Stretch
Face a wall directly, walking your fingers up progressively to capture incremental forward flexion stretch. Hold the peak terminal point for 30 seconds to accurately mark structural progress over weeks.
External Rotation Stretch
Utilize doorway parameters or stick-assisted mechanics. Adhesive capsulitis exercises must include external rotation, as it targets the most structurally restricted joint motion field. Hold for 30-60 seconds.
Overhead Pulley Care
Deploy an overhead pulley system, using the healthy opposite arm to gently assist and guide the affected arm overhead. Provides a highly controlled, progressive, non-traumatic joint envelope stretch.
Safety Control Rule: Stretches should take the shoulder strictly to the point of discomfort, but NEVER into sharp pain. Specialized physical therapy ensures structural technique optimization and prevents secondary reactive bursitis inflammation.